








A New Demand for Justice in Sickle Cell Disease
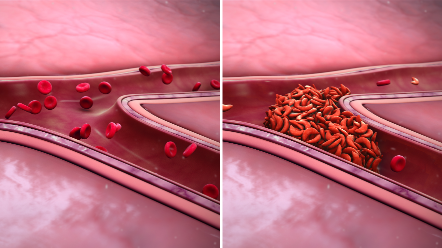
Sickle cell disease (SCD) is an inherited blood disorder that alters the shape of red blood cells. Instead of being round and flexible, the cells become C-shaped, rigid, and sticky, which can slow or block circulation. One of the most common symptoms is severe, incapacitating pain—known as sickle cell crises—that often sends patients to the emergency room and can manifest as acute flares or persist as chronic pain for years.
SCD affects over 100,000 people in the United States. Although it is considered an orphan disease, it remains one of the most common genetic disorders diagnosed in the country, with its prevalence continuing to rise. Nevertheless, patients with SCD are frequently overlooked by the healthcare system and are often regarded as “forgotten patients,” largely due to a lack of understanding about the condition, racial prejudice, and harmful assumptions regarding patients’ motivations for seeking pain management.
The final panel of the 2025 Galien Patient Summit addressed the challenges of diagnosing and treating SCD. Moderated by Jeremy Abbate of Scientific American, the panel featured SCD patient Dr. Melissa Creary from the University of Michigan, Dr. Ify Osunkwo from Novo Nordisk, Dr. Olivier Hermine from Necker Hospital in Paris, and Dr. Solomon F. Ofori-Acquah from Emory
University. The discussion was sparked by a question from an audience member: “Sickle cell disease has been a model for scientific discovery for all diseases. How can we create a new model for patient involvement and advocacy to lead the way for other rare diseases?”
The Problem with Being the "Model"
Dr. Ofori-Acquah noted that SCD has long been a considered model, often to its detriment. SCD has been a model for a long time, yet it remains very challenging in terms of care,” he said. He highlighted that SCD was foundational in understanding gene regulation and was a target for early gene therapy attempts, ultimately leading to the 2023 approval of Casgevy and Lyfgenia, the first gene therapies for SCD.
However, Dr. Ofori-Acquah argued that despite it status as a model, the field has yet to see substantial benefits. “We’ve been a model for a long time and haven’t received much in return,” he said. “Before we elevate it as a model for another paradigm, we need to see some benefits.”
Dr. Osunkwo agreed, suggesting that the community should be “excused” from this burden. “We’ve served a model for science long enough,” she said. “It’s time we benefit from someone else’s model that has proven effective.”
She proposed looking at HIV as a model for SCD. “HIV faces a stigma, has a multisystem impact, and is globally widespread,” she said. “What worked was that the community transitioned from dealing with stigma to becoming an empowered patient group that drove innovation and improved treatment access. They also leveraged intersectionality.”
Trust, Justice, and Data
For Dr. Creary, who has lived with SCD since a young age, the community faces a crisis of justice. “We must openly address specific needs of particular populations,” she said. “When we center justice, we begin to realize that we can’t make assumptions about what justice should look like without genuinely engaging with the patient population.”
This engagement, she argued, must acknowledge the existing lack of trust. "How do we understand the trust that has been broken over decades?" Dr. Creary asked." We must first recognize and honor the distrust that is already present."

Part of that distrust arises from the misuse of data. “As a patient population, we need to understand the power of data, how to mobilize around it, and use it for our benefit,” Dr. Creary said. “We must form partnerships to ensure that data usage benefits us, which means engaging
in open conversations with partners and ourselves to clarify what the data is and how we can utilize it.”
This requires a fundamental shift in perspective, moving beyond lab values to consider lived experiences. Dr. Hermine, a hematologist at Necker Hospital in Paris, stressed that physicians often overlook the true burden of SCD. “When a patient experiences pain, it can significantly impair their quality of life, work capacity, and social interactions,” he said. “However, the perception of that impairment must come from the patient to capture the full picture.”
The Global Reality and a New Path
The panel repeatedly consistently emphasized that this is a global issue. "There are 8 million people with sickle cell disease worldwide,” said Dr. Osunkwo. “That equates to approximately 1,024 deaths daily."
This global disparity is a source of deep frustration. Dr. Ofori-Acquah, who is from Ghana, noted that in West Africa, "one out of every 50 live births has sickle cell disease." Yet, he pointed out that while immunization rates in these countries are nearly perfect, there is no newborn screening for SCD. “If we invest in regions where the disease is endemic, we enhance centers of excellence and build infrastructure to better understand the disease; that is our path to meaningful community engagement,” he said.
With a life expectancy gap of 20 to 30 years for SCD patients, the panelists outlined the way
forward:
- Dr. Ofori-Acquah: “Let's close the gap by actively engaging the global community. When someone asks, "Do you know your status?' it shouldn" just be about HIV; it should include about sickle cell disease.”
- Dr. Hermine: “We need education for patients, physicians, scientists, regulators, and industry partners.”
- Dr. Osunkwo: “Innovation. Utilize AI. Leverage what others have done and determine how to apply it to SCD.”
Dr. Creary was given the final word. Her response was bracing, direct, and left no room for ambiguity. "We must confront systemic racism,” she said. “We must address health equity honestly. We need to recognize what we're offering this hyper-marginalized community and not ignore it."
A recording of this Galien Patient Summit panel can be viewed here.